
Effectiveness of Ventilation via an Endotracheal Tube in Pharynx Versus a Facemask in Patients With Potentially Difficult Airway: A Randomized, Crossover, and Blind Trial
The success rate of ventilation with an end endotracheal tube in the pharynx is similar to face mask ventilation in adult patients at risk for difficult airways.

Takeaway
The success rate of ventilation with an end endotracheal tube in the pharynx is similar to face mask ventilation in adult patients at risk for difficult airways.
Key Points
- Studied success rates of ventilation in adults with potentially difficult airways (BMI>30 kg/m 2 , and/or Mallampati class III or IV)
- Successful ventilation was defined as CO2 observed at least once on capnography within the initial 3 consecutive attempted breaths
- Inclusion criteria include >18 years, requiring general anesthesia with tracheal intubation, BMI >30 kg/m 2 , and/or Mallampati class III or IV.
- Exclusion criteria include acute and chronic respiratory disorders (including chronic obstructive lung disease (COPD) and asthma), ASA classification ≥ IV, emergency surgery, induction requiring rapid sequence induction, patients requiring awake intubation, pregnant women, and contraindication for mask ventilation.
- Depth of the endotracheal tube was measured length from the ear canal to upper incisor
- Once the tube reached the target depth, the seal at the lips was achieved with a 2-hand techniqu
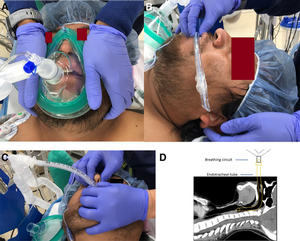
- Mask ventilation performed without nasal or oral airway
Excerpts
The extreme condition of a difficult airway is a “cannot intubate and cannot oxygenate (CICO)” scenario, which occurred at an incidence of 0.003%,4 accounting for 25% to 28% of patient deaths in the perioperative setting.
success rate of emergency front-of-the-neck access when performed by even experienced anesthesiologists in perioperative settings is only 35%.
The airway obstruction in an unconscious individual most likely occurs in the upper airway15–17 due to pharyngeal dilator muscle paralysis, soft palate, tongue, and upper glottis blockage.
Theoretically, an endotracheal tube in the pharynx (TTIP) can bypass the tongue, soft palate, and epiglottis, potentially overcoming airway obstruction.
Overall, the success rates of TTIP and mask ventilation were 93.4% (127/136) and 84.6% (115/136), respectively ( P = .02). In the sequence of Tube first, 7 (9.9%) out of 71 patients failed Step 1 ventilation with TTIP. Of these 7 patients, 6 (85.7%) were successfully rescued with mask ventilation. In the sequence of mask first, 13 (20.0%) out of 65 patients failed mask ventilation. All 13 patients (100%) were successfully rescued with TTIP ventilation.
this technique can be utilized in a patient with limited mouth opening. A patient only needs to have a mouth opening wide enough to allow passage of an endotracheal tube. It is important to emphasize that for an individual with a relatively small oro-pharyngeal cavity, SGA insertion may be impossible. An oral airway may push the tongue downward and worsen airway obstruction. Third, successful ventilation is independent of an adequate mask seal, which is required for mask ventilation.
This study demonstrated that the success rate of TTIP ventilation is higher than that of the mask ventilation (2-hand V-E technique) without an oral or nasal airway insertion in patients with a potentially difficult airway.
positive pressure applied to the pharynx via TTIP creates an upward pressure gradient between the pharynx and the oral cavity. Such an upward pressure gradient would not worsen the upper airway obstruction. However, during classic mask ventilation, a downward pressure gradient exists between the oral cavity and the glottis with or without an oral airway. Such a downward pressure gradient may worsen airway obstruction
it is warranted to conduct large-scale clinical trials to assess the effectiveness of using TTIP as a rescue technique for failed SGA or mask ventilation with an oral or nasal airway insertion
Abstract
Background:
The difficult airway is frequently encountered across many scenarios. The extreme form is a "cannot intubate and cannot oxygenate" scenario, which lacks a reliable rescue technique. Previous case reports or studies with small sample sizes indicate the feasibility and efficiency of an endotracheal tube in the pharynx (TTIP) to ventilate patients. We hypothesize that ventilation via TTIP is an effective rescue technique for failed mask ventilation.
Method:
One hundred forty-seven patients with potentially difficult airways were randomly assigned to the sequence (Tube first) of tube first ventilation via TTIP for 1 minute after induction, followed by via mask ventilation for 1 minute or in reverse sequence (Mask first). The ventilation was done with pressure control mode, a peak inspiratory airway pressure of 20 cmH2O, an inspiratory to expiratory time ratio of 1:2, and a respiratory rate of 10 breaths/min.
Results:
A total of 136 patients underwent final analysis. The overall success rate (primary outcome) of ventilation via TTIP and mask, defined as the presence of expired carbon dioxide, was 93.4% (127/136) and 84.6% (115/136), respectively (P = .02). The success rate, 85.7% (6/7), of mask ventilation rescuing a failed TTIP ventilation and 100% (13/13) of TTIP rescuing a failed mask ventilation were comparable (P = .35).
Conclusions:
The success rates of TTIP and mask ventilation are comparable. Ventilation via TTIP could be an alternative rescue technique for managing a difficult airway.
Citation
Markham T, AlFarra AS, Tejani M, Tate DJ, Barrera JE, Paladugu S, Saroukhani S, Jiang Y. Effectiveness of Ventilation via an Endotracheal Tube in Pharynx Versus a Facemask in Patients With Potentially Difficult Airway: A Randomized, Crossover, and Blind Trial. Anesth Analg. 2024 Dec 20. doi: 10.1213/ANE.0000000000007273. Epub ahead of print. PMID: 39705182.